Selina Begum - a 21yr old female university student brought in by ambulance due to acute-onset abdominal pain and vomiting. She is lethargic. Selina has been feeling under the weather recently, which she thinks was just a common cold. She is otherwise well.
On further questioning:
HR 102, BP 105/76, RR 24, SpO2 95% OA, Temp 37.2C, Lethargic/Confused
Examination
Selina is talking. Her airway is patent and self-maintaining.
Investigations
None required.
Interventions
None required.
Examination
RR: 24, SpO2: 95%
Chest expansion – normal and equal
Percussion - normal resonance
Auscultation - good air entry bilaterally with no added sounds
Investigations
None required.
Interventions
None required.
Examination
HR 100, BP 98/74, Temp 36.5C
Pulse is fast, regular, but feels weak
CRT 4 seconds
HS I + II + 0
No peripheral oedema
If asked about urine output – you’ve not been all day – but the previous couple of days had actually been going to the toilet a lot
Dry mucous membranes
Investigations
Insert at least one wide-bore cannula – 14G (Orange) or 16G (Grey)
Bloods – ask to justify:
Urinalysis for glucose and ketones
VBG - no hypoxia, so no need for arterial sample
12-lead ECG
Consider 'sepsis six' screen
Interventions
Patient is hypovolaemic
If raised glucose and ketones - ?DKA
Until investigations come back, students should consider sepsis as a possible cause and begin treatment with empiric antibiotics. These can be stopped once sepsis is ruled out.
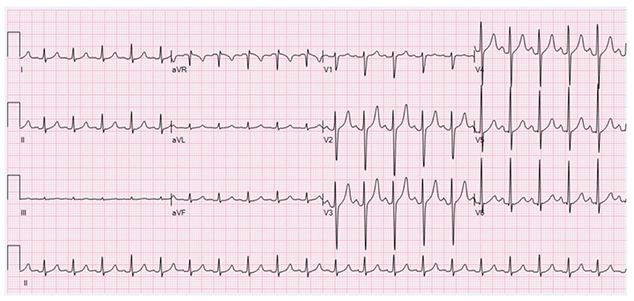
This ECG shows sinus tachycardia.
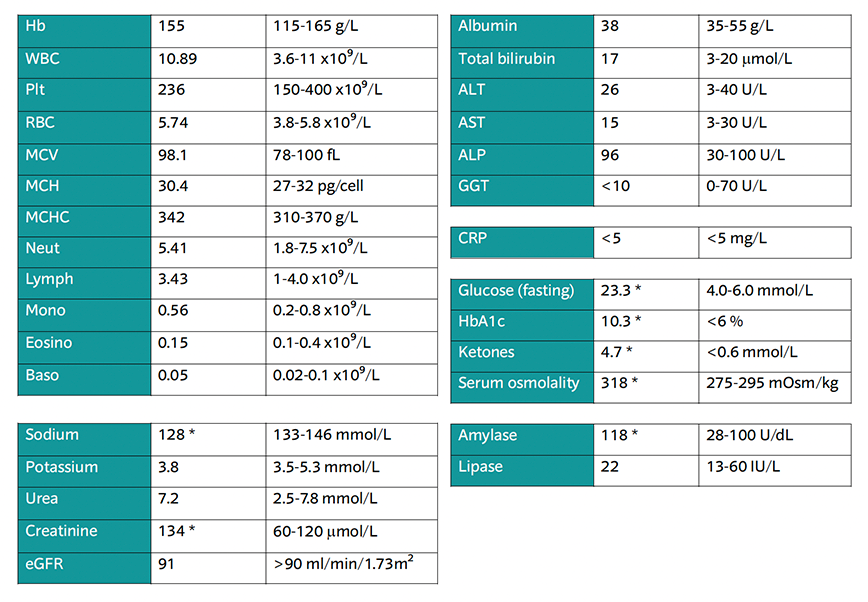
Glucose, HbA1c ketones and serum osmolality are elevated - this fits with the picture of diabetic ketoacidosis
The patient has an electrolyte abnormality, likely related to dehydration, and raised amylase, which can happen due to acidosis
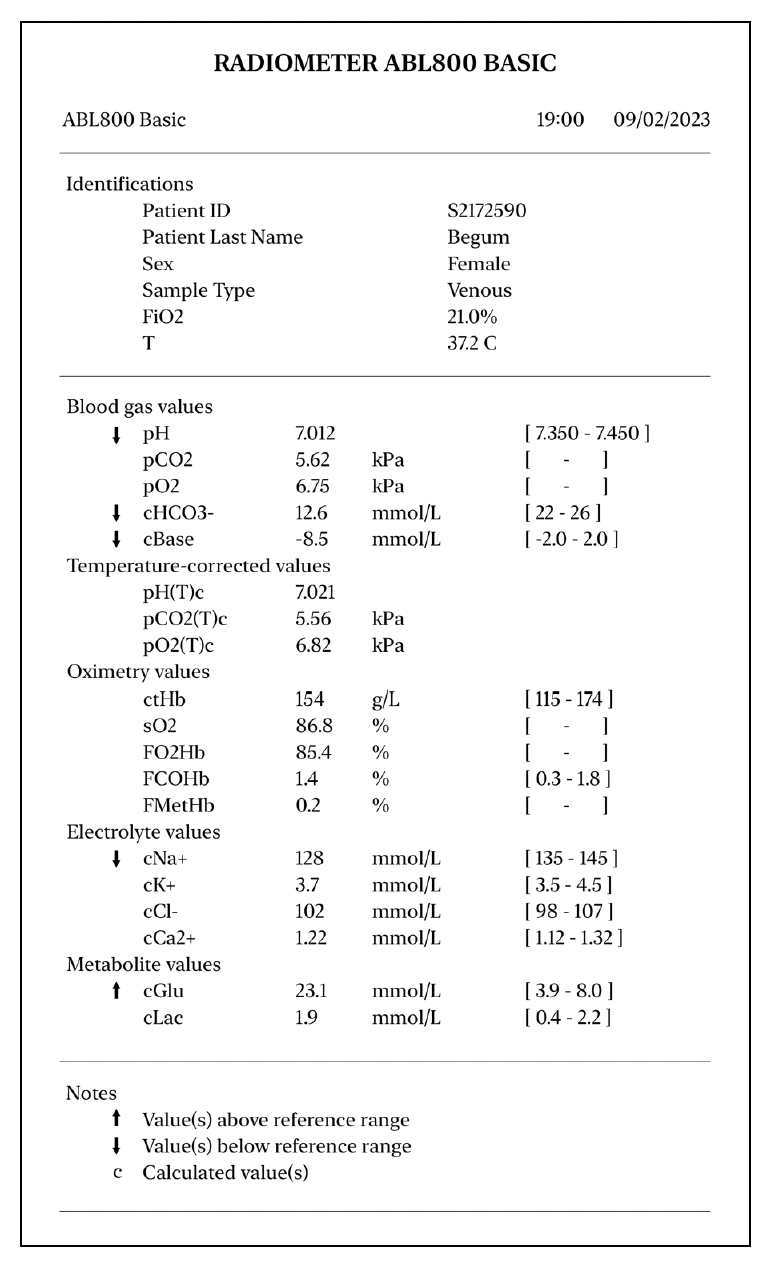
Metabolic acidosis
Cannot comment on respiratory compensation due to venous sample
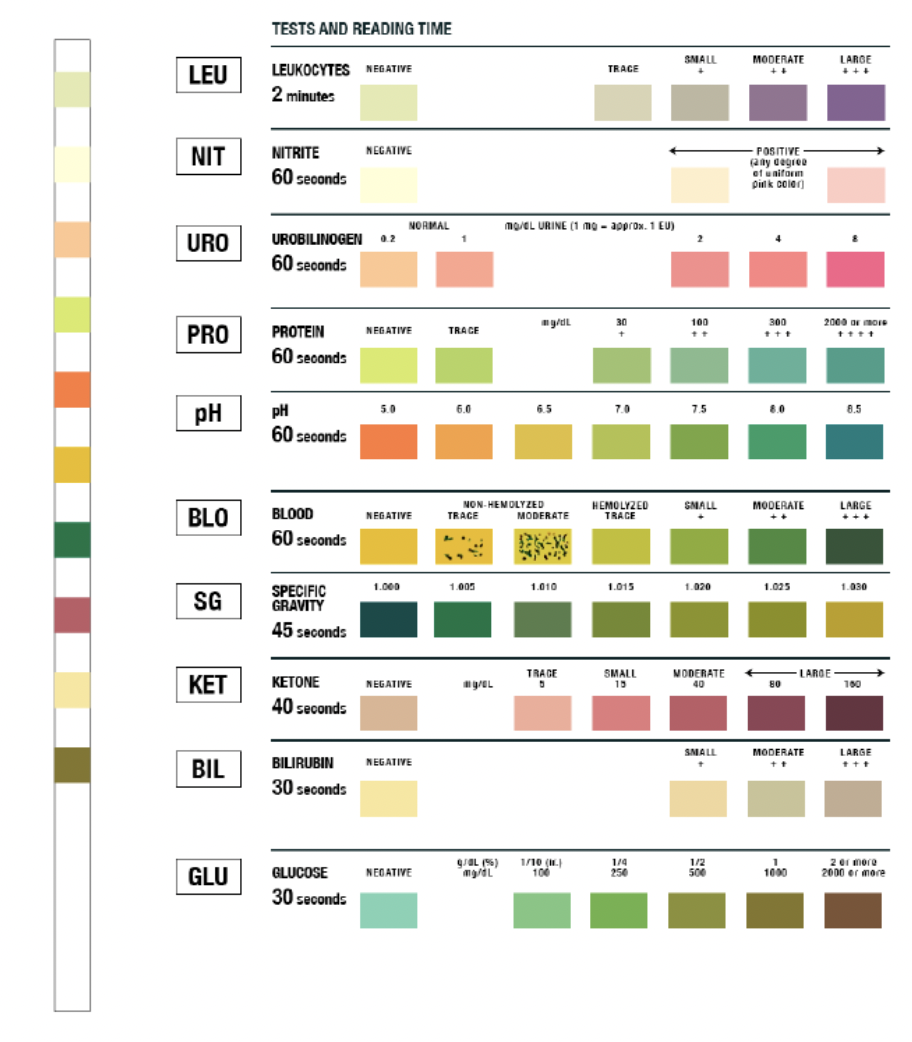
Ketones present (moderate)
Glucose present (1000 mg/dL)
Examination
Alert but tired/irritable
GCS 14/15 – E3 V5 M6
PEARL
If students perform neurological exam – Selina is weak and lethargic, no cranial nerve findings
Investigations
Bedside CBG if not already performed in C – 23.3 mmol/L
Bedside ketones – 4.7 mmol/L
Interventions
IV NaCl with K+ and FRIII as above
Examination
No skin findings
Abdomen is very tender to palpation with mild guarding. No distention. Normal bowel sounds
Calves SNT
No peripheral oedema
Selina doesn’t think she could be pregnant
She hasn’t taken any drugs or alcohol
Investigations
Consider PR exam - NAD
Consider abdominal imaging to rule out acute abdomen (bedside USS would be most appropriate, or arrange CTAP) - NAD
Urine pregnancy test - negative
Consider toxicology screen - NAD
Interventions
Provide analgesia in accordance with pain ladder
Can you confirm a diagnosis?
What will you do now?
Leicester Wilderness and Emergency Medicine Society
University of Leicester Medical School, University Road, LE1 7RH, UK
Follow us on:
© Leicester Wilderness and Emergency Medicine Society
In partnership with:
![]()
![]()
![]()